By Jennifer Swink | Celebrity Skin Scottsdale
Dark spots are one of the most common reasons people seek professional skincare treatment, yet many people don’t know exactly what type of pigmentation they have. Melasma and post-inflammatory hyperpigmentation (PIH) can look surprisingly similar, but they develop for completely different reasons. Melasma is primarily influenced by hormones, sun exposure, visible light, heat, and genetics, while post-inflammatory hyperpigmentation develops after inflammation caused by acne, eczema, injuries, burns, or cosmetic procedures. Because the underlying causes are different, the treatments that work best are different as well.
Receiving the correct diagnosis is one of the most important steps toward achieving clearer, more even-toned skin. Treating the wrong condition can delay improvement, waste money on ineffective products, and in some cases make pigmentation more difficult to manage. This is especially true for individuals with medium to darker skin tones, who naturally produce more melanin and are more susceptible to developing excess pigmentation after inflammation.
In this article, you’ll learn how to tell the difference between melasma and post-inflammatory hyperpigmentation, why proper diagnosis matters, and what treatment options may help restore a more even complexion.
Table of Contents
Quick Answer
Melasma vs. post-inflammatory hyperpigmentation (PIH) can look similar, but melasma is usually triggered by hormones, ultraviolet (UV) radiation, visible light, heat, and genetics, while post-inflammatory hyperpigmentation develops after inflammation from acne, eczema, injuries, burns, or cosmetic procedures. Because the underlying causes are different, the most effective treatments are different. Correct diagnosis is the first step toward choosing the right skincare products, professional treatments, and long-term management plan.
Why Correct Diagnosis Matters
Although melasma and post-inflammatory hyperpigmentation both appear as darker areas of skin, they are fundamentally different conditions. Melasma is considered a chronic pigment disorder, whereas post-inflammatory hyperpigmentation is the skin’s natural response to inflammation or injury. Understanding which condition you have helps determine everything from your skincare products to the professional treatments that are most appropriate.
For example, someone with acne-related PIH may see significant improvement once inflammation is controlled and pigment-producing cells gradually return to normal. Melasma, on the other hand, often requires ongoing management because hormonal influences, ultraviolet radiation, visible light, and heat continue to stimulate pigment production even after the discoloration has faded.
Researchers now understand that melasma is far more complex than excess melanin alone. Studies have found changes involving inflammation, increased blood vessel formation, disruption of the skin barrier, and abnormal melanocyte activity, helping explain why melasma often returns if its triggers are not carefully managed. This complexity is one reason why successful treatment usually requires a combination of professional care, medical-grade skincare, and diligent sun protection rather than a single treatment alone
What Is Melasma?
Melasma is a chronic skin condition that causes patches of brown, gray-brown, or tan discoloration, most commonly on the cheeks, forehead, upper lip, nose, and chin. Unlike many other forms of pigmentation, melasma usually appears in a symmetrical pattern, affecting both sides of the face.
Melasma is sometimes called the “mask of pregnancy” because hormonal changes during pregnancy commonly trigger the condition. However, pregnancy is only one possible cause. Birth control pills, hormone replacement therapy, menopause, genetics, ultraviolet (UV) radiation, visible light, and heat exposure can all contribute to its development. Even people who carefully avoid direct sunlight may experience flare-ups because visible light and heat alone can stimulate pigment-producing cells.
According to the American Academy of Dermatology, melasma affects women far more often than men and is particularly common in individuals with Fitzpatrick skin types III through VI, including Hispanic, Asian, Middle Eastern, and African American populations.
One reason melasma can be frustrating is that the pigment often extends deeper into the skin than many people realize. Some cases involve primarily epidermal pigment, while others include pigment deeper within the dermis or a combination of both. This variation partly explains why some individuals respond quickly to treatment while others require longer-term management.
Unlike age spots, which usually develop after years of cumulative sun exposure, melasma tends to appear as larger patches with softer borders rather than isolated individual spots. It also has a much greater tendency to recur if the underlying triggers are not addressed.

Common melasma triggers include:
- Hormonal changes
- Pregnancy
- Birth control pills
- Hormone replacement therapy
- Menopause
- Ultraviolet (UV) radiation
- Visible light
- Heat exposure
- Genetic predisposition
- Certain medications and cosmetics
Many people are surprised to learn that melasma is not simply a cosmetic concern. Research has shown that the condition involves inflammatory pathways, vascular changes, and alterations to the skin barrier in addition to increased melanin production. This is one reason treatment often requires patience and a comprehensive approach rather than relying on a single cream or procedure.
What Is Post-Inflammatory Hyperpigmentation (PIH)?
Post-inflammatory hyperpigmentation (PIH) develops after the skin experiences inflammation or injury. Rather than being caused by hormones, PIH is the result of the skin’s natural healing response. When inflammation occurs, melanocytes—the cells responsible for producing pigment—become overstimulated and create excess melanin. As the skin heals, this extra pigment remains behind as a flat brown, gray, or black mark.
Unlike melasma, PIH appears exactly where inflammation occurred. Acne is the most common cause, but eczema, psoriasis, insect bites, burns, cuts, allergic reactions, waxing, aggressive cosmetic procedures, and even picking at the skin can all leave behind post-inflammatory hyperpigmentation.
PIH can affect anyone, but it is significantly more common and often more persistent in individuals with medium to darker skin tones. Research has shown that melanocytes in darker skin are more reactive following inflammation, increasing the likelihood of excess pigment production after even relatively minor skin injuries.
Unlike melasma, PIH is not usually symmetrical. Instead, the discoloration follows the exact pattern of the inflammation that caused it. For example, someone with acne may notice individual dark spots where each blemish healed, while someone who experienced eczema may develop larger irregular patches in the affected areas.
The encouraging news is that PIH often improves once the underlying inflammation is controlled. Although fading may take several months—and sometimes longer depending on the depth of the pigment and your skin tone—the condition generally has a more predictable course than melasma when managed appropriately.
Common causes of post-inflammatory hyperpigmentation include:
- Acne
- Picking pimples
- Eczema
- Psoriasis
- Insect bites
- Burns
- Cuts and scrapes
- Cosmetic procedures
- Waxing
- Laser treatments
- Chemical irritation
One of the biggest mistakes people make is focusing only on the discoloration while ignoring the inflammation that caused it. Continuing to develop acne breakouts, repeatedly picking at blemishes, or using irritating skincare products can trigger new pigmentation faster than old spots have time to fade.
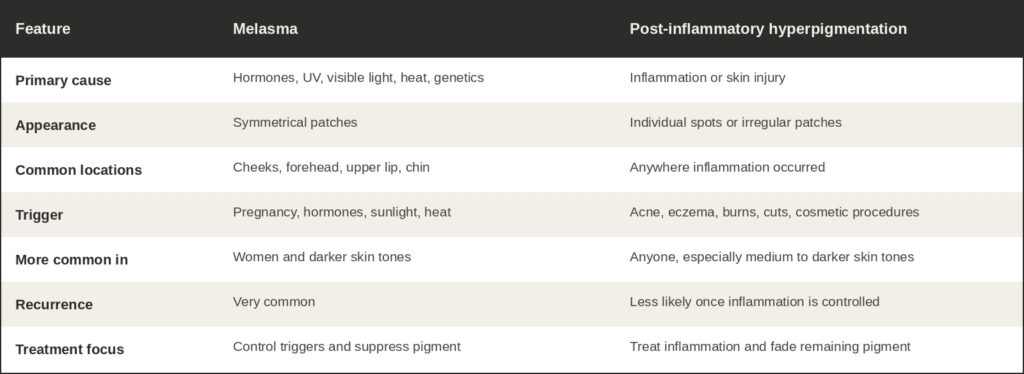
Melasma vs. Post-Inflammatory Hyperpigmentation at a Glance
Could It Be Something Else?
Although melasma and post-inflammatory hyperpigmentation (PIH) are among the most common causes of facial discoloration, they are not the only reasons brown spots develop. A proper diagnosis is important because each condition has different causes and treatment approaches.
Age Spots (Solar Lentigines)
Age spots, also called solar lentigines, develop after years of cumulative ultraviolet (UV) exposure. They usually appear as individual round or oval brown spots with well-defined borders on the face, chest, shoulders, forearms, and backs of the hands. Unlike melasma, they are not caused by hormones and are generally easier to treat because there is no ongoing trigger continually stimulating pigment production.
Freckles (Ephelides)
Freckles are inherited and typically appear during childhood. They become darker with sun exposure and often fade during the winter months. Unlike melasma or PIH, freckles are not caused by inflammation or hormonal changes.
Drug-Induced Hyperpigmentation
Certain medications can stimulate pigment production or increase sun sensitivity, leading to discoloration. If pigmentation develops after starting a new medication, consult your healthcare provider before making any changes.
Other Pigment Disorders
Less common pigment disorders can also cause facial discoloration. In addition, any spot that rapidly changes in size, shape, color, or begins to bleed should be evaluated by a dermatologist to rule out skin cancer or another serious condition.
Can You Have More Than One Type of Pigmentation?
Yes. In fact, many people have multiple forms of pigmentation at the same time.
For example, someone may have melasma across the cheeks, post-inflammatory hyperpigmentation from acne along the jawline, and age spots from years of sun exposure on the forehead or hands.
Because each condition develops differently, every type of pigmentation may require a different treatment strategy. Treating every brown spot the same way often leads to disappointing results. A professional skin evaluation helps identify the underlying causes so your treatment plan can be customized specifically for your skin.
Why Pigmentation Treatments Sometimes Fail
One of the biggest reasons pigmentation doesn’t improve is that the underlying cause has never been addressed.
The Wrong Diagnosis
Melasma is often mistaken for acne marks, while PIH is frequently assumed to be melasma. Since each condition responds differently to treatment, using the wrong approach can slow progress and increase frustration.
Treating Only the Pigment
Pigment is the result—not the cause.
If acne continues to produce inflammation, new PIH will continue to form. Likewise, if hormonal changes, UV exposure, visible light, or heat continue triggering melasma, the pigmentation often returns even after successful treatment.
Inconsistent Sun Protection
Daily broad-spectrum sunscreen is one of the most important parts of treating pigmentation. Research shows that ultraviolet radiation and visible light both contribute to melasma. Tinted mineral sunscreens containing iron oxides provide additional protection against visible light and may help reduce recurrence.
Aggressive Treatments
Stronger isn’t always better. Overly aggressive chemical peels, lasers, or skincare products can create additional inflammation, increasing the risk of more pigmentation—especially in medium to darker skin tones. A gradual, personalized approach often produces safer, more predictable results.
Expecting Immediate Results
Pigmentation takes time to fade. Depending on the diagnosis, skin tone, and depth of pigment, noticeable improvement may require several months of consistent home care and professional treatment.
Professional Treatments and Skincare That May Help
Successfully treating melasma and post-inflammatory hyperpigmentation isn’t simply about removing pigment—it’s about improving the skin without creating unnecessary inflammation that can trigger even more pigment production. This is especially important with melasma, where heat, inflammation, ultraviolet (UV) light, and even certain cosmetic procedures may stimulate melanocytes and worsen discoloration.
For this reason, successful treatment is rarely about choosing the strongest procedure. A conservative, progressive approach often produces safer, more predictable, and longer-lasting results. Starting with gentler treatments allows your skin’s response to be evaluated before gradually increasing treatment intensity when appropriate. While this approach is particularly important for individuals with melasma and medium to darker skin tones, it often produces better long-term outcomes for all skin types.
One of the most important concepts to understand is this:
The goal isn’t to create as much inflammation as possible—it’s to create just enough controlled stimulation to encourage healthier skin while minimizing the risk of excess pigment production.
Professional treatments achieve the best results when combined with medical-grade skincare, diligent sun protection, and a personalized home-care routine.
Professional Skincare Products
Professional skincare is the foundation of nearly every successful pigmentation treatment plan. While many over-the-counter products advertise the same active ingredients, they are not necessarily formulated the same way. Ingredient concentration, stability, pH, delivery systems, supporting ingredients, and overall formulation all influence how effectively a product performs.
Depending on your diagnosis, ingredients such as vitamin C, retinoids, azelaic acid, tranexamic acid, niacinamide, kojic acid, cysteamine, and carefully supervised hydroquinone may be recommended. Selecting the right ingredients—and using them consistently—is often more important than simply using more products. Because every type of pigmentation responds differently, a professional skin consultation can help determine which ingredients and treatment plan are most appropriate for your specific skin concerns.
Chemical Peels
Professional chemical peels can be highly effective for improving both melasma and post-inflammatory hyperpigmentation by increasing skin cell turnover and gradually reducing excess pigment. However, selecting the appropriate peel—and the appropriate timing—is critical.
For many patients, especially those with melasma, beginning with lighter or superficial peels before progressing to medium-depth peels allows the skin to build tolerance while minimizing unnecessary inflammation. Although medium-depth peels can produce excellent results in carefully selected patients, starting conservatively and progressing gradually is often the safest approach regardless of skin tone.
Equally important is proper skin preparation. Pre-treatment skincare helps reduce inflammation, stabilize melanocyte activity, strengthen the skin barrier, and prepare the skin for treatment. After a peel, post-treatment products support healing and help reduce the risk of rebound pigmentation. This comprehensive approach often produces more consistent, long-term improvement than relying on procedures alone.
Microneedling
Microneedling can improve acne scars, fine lines, skin texture, and certain types of pigmentation. Patients with post-inflammatory hyperpigmentation often benefit once active inflammation has been controlled. For melasma, treatment should be approached conservatively and combined with pigment-suppressing skincare to help reduce the risk of flare-ups.
Clear + Brilliant®
Clear + Brilliant® is a gentle fractional laser that stimulates healthy skin renewal while improving uneven skin tone, texture, and early sun damage. In carefully selected patients, it may also improve certain types of pigmentation.
Like chemical peels, the goal is not to perform the most aggressive treatment possible. Multiple conservative treatments often produce more natural, predictable improvement than one aggressive procedure, particularly for patients with melasma or those prone to developing post-inflammatory hyperpigmentation.
Because heat may trigger melasma in some individuals, patient selection, treatment settings, and proper pre- and post-treatment skincare are essential.
LED Light Therapy
LED Light Therapy does not directly remove pigmentation, but it can help reduce inflammation and support the skin’s natural healing response. It is often combined with procedures such as chemical peels, microneedling, and Clear + Brilliant® to promote recovery while supporting healthier skin.
A Personalized, Progressive Approach
No two pigmentation cases are exactly alike. Some patients respond beautifully to conservative treatments alone, while others benefit from gradually incorporating more advanced procedures as their skin becomes healthier and more resilient.
Rather than asking, “What is the strongest treatment?” a better question is, “What is the safest and most effective treatment for my skin right now?”
A progressive treatment plan that combines professional procedures, medical-grade skincare, daily sun protection, and ongoing maintenance often provides the most predictable long-term improvement while minimizing the risk of triggering additional pigmentation.
How to Help Prevent Pigmentation From Returning
While no treatment can permanently eliminate every form of pigmentation, daily habits play a significant role in preventing recurrence.
- Apply a broad-spectrum SPF 30 or higher every day.
- If you have melasma, consider a tinted mineral sunscreen containing iron oxides to help protect against visible light.
- Wear a wide-brim hat and seek shade whenever possible.
- Treat acne and other inflammatory skin conditions promptly.
- Avoid picking blemishes or scratching irritated skin.
- Protect your skin barrier by avoiding excessive irritation from harsh skincare products.
- Continue using your maintenance skincare even after your pigmentation improves.
Remember, pigmentation management is a marathon—not a sprint. Consistency with your skincare routine, sun protection, and professional treatments is often what separates temporary improvement from long-term success.
When to Schedule a Professional Skin Evaluation
If you’re unsure whether you’re dealing with melasma, post-inflammatory hyperpigmentation, age spots, or another form of pigmentation, a professional skin evaluation can help identify the underlying cause.
At Celebrity Skin Scottsdale, every treatment plan begins with understanding why your pigmentation developed. By combining professional treatments, medical-grade skincare, and personalized recommendations, we work to improve existing discoloration while helping reduce the likelihood of future pigmentation.
Conclusion
Melasma and post-inflammatory hyperpigmentation may look similar, but they are very different conditions with different causes, triggers, and treatment strategies. Correct diagnosis is one of the most important steps toward achieving clearer, healthier-looking skin.
Whether your pigmentation developed after acne, pregnancy, years of sun exposure, or another trigger, successful treatment involves addressing both the visible discoloration and the underlying cause. With the right combination of professional care, medical-grade skincare, sun protection, and patience, significant improvement is often possible.
Frequently Asked Questions
Is melasma the same as post-inflammatory hyperpigmentation?
No. Melasma is primarily influenced by hormones, UV radiation, visible light, heat, and genetics, while post-inflammatory hyperpigmentation develops after inflammation or injury.
Can you have both conditions?
Yes. Many people have melasma along with acne-related PIH or age spots, requiring a customized treatment plan.
Which is harder to treat?
Melasma is generally more challenging because it is chronic and influenced by ongoing triggers. PIH often improves once inflammation is controlled and the excess pigment gradually fades.
Are chemical peels safe for darker skin?
Yes, when the correct peel is selected and performed by an experienced professional. Treatment should always be customized to reduce the risk of additional pigmentation.
How long does it take to see improvement?
Some people notice improvement within several weeks, while others require several months depending on the diagnosis, depth of pigmentation, skin tone, and consistency with treatment.
Does sunscreen really matter?
Absolutely. Daily sun protection is one of the most important steps in treating and preventing both melasma and post-inflammatory hyperpigmentation.
